Myelodysplastic/myeloproliferative neoplasm with neutrophilia (MDS/MPN-N)
- Method:
- Anticoagulant:
- Recommendation:
- Method:Cytomorphology
- Anticoagulant:EDTA
- Recommendation:obligatory
- Method:Immunophenotyping
- Anticoagulant:EDTA or Heparin
- Recommendation:facultative
- Method:Chromosome analysis
- Anticoagulant:Heparin
- Recommendation:obligatory
- Method:FISH
- Anticoagulant:
- Recommendation:no
- Method:Molecular genetics
- Anticoagulant:EDTA or Heparin
- Recommendation:obligatory
Based on the current guidelines and the current state of research, there are different diagnostic recommendations for patients with MDS/MPN-N (myelodysplastic /myeloproliferative neoplasm with neutrophilia). We have summarized the most important information on classification and diagnostic methods at MLL.
MDS/MPN-N: Classification
Myelodysplastic/myeloproliferative neoplasm with neutrophilia (MDS/MPN-N) is a myeloid neoplasm with myelodysplastic and myeloproliferative features characterized by persistent neutrophilia in peripheral blood and neutrophilic left-shift (Khoury et al. 2022). The name MDS/MPN-N was introduced in 2022 with the appearance of the new WHO classification, replacing in it the designation of the entity as atypical chronic myeloid leukemia (aCML), BCR::ABL1-negative. The change in name emphasizes the myelodysplastic/myeloproliferative nature of the disease and is intended to avoid confusion with chronic myeloid leukemia (CML) (Khoury et al. 2022). In the International Consensus Classification (ICC), also published in 2022, the entity is referred to as atypical chronic myeloid leukemia (Arber et al. 2022).
Table 1: Diagnostic criteria in MDS/MPN-N (Khoury et al. 2022)
|
Essential:
|
|
Desirable:
|
* Diagnosis of MDS/MPN-N requires exclusion of a BCR::ABL1 fusion gene, which requires careful evaluation to exclude cryptic rearrangements and/or alternate BCR::ABL1 transcripts using available methods (e.g., cytogenetics, fluorescence in situ hybridization, or PCR-based analyses).
** Mutations in these genes are uncommon in MDS/MPN-N and should prompt morphologic examination to rule out alternative diagnoses.
MDS/MPN-N: Diagnostic methods and their relevance
Cytomorphology is used for differentiation from the other myeloproliferative disorders (MPN), CMML and myelodysplastic neoplasm (MDS) and for confirming the diagnosis. It is also required for classification according to WHO.
Aberrant karyotypes occur in 30-40% of cases, with trisomy 8 being the most common chromosomal aberration. Other recurrent chromosomal aberrations include monosomy 7, or 7q deletion, isochromosome 17q, and loss of the Y chromosome. In addition, complex aberrant karyotypes may be present (Meggendorfer et al. 2018, Khoury et al. 2022, Patnaik & Tefferi 2023).
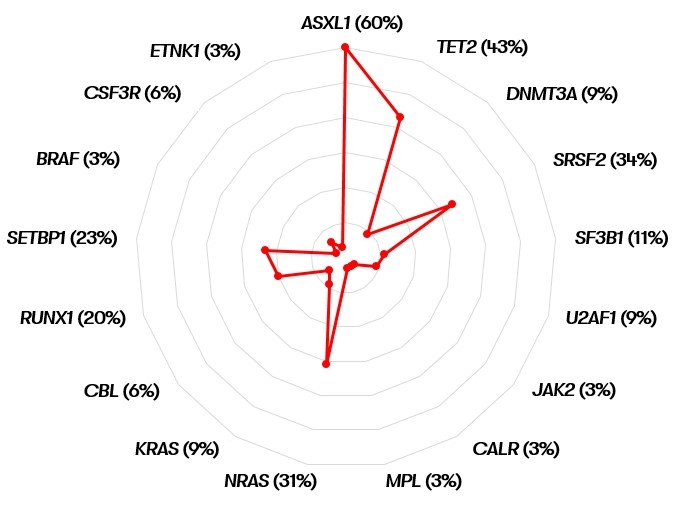
Molecular genetics can be used to detect commonly occurring mutations in MDS/MPN-N, which are summarized in Figure 1. While ASXL1, TET2, and SRSF2 are most commonly mutated but also occur in other myelodysplastic/myeloproliferative neoplasms, the presence of a SETBP1 and/or ETNK1 mutation supports the diagnosis of MDS/MPN-N (Meggendorfer et al. 2013, Piazza et al. 2013, Zoi & Cross 2015, Meggendorfer et al. 2018). Mutations in the ASXL1 and SETBP1 genes are associated with an unfavorable prognosis (Meggendorfer et al. 2013, Zoi & Cross 2015). Differential diagnosis of chronic neutrophil leukemia (CNL) should be considered in the presence of a mutation in CSF3R (Khoury et al. 2022). Mutations in CSF3R and JAK2 also allow specific therapy.
MDS/MPN-N: Prognosis
The median survival of MDS/MPN-N patients is 14-29 months (Khoury et al. 2022). However, because it is a rare disease, there is no uniform consensus on risk stratification (Patnaik & Tefferi 2023). As a prognostic-negative parameter in MDS/MPN-N, a leukocyte count of >50x109 /L has been described in several studies (Onida et al. 2002, Breccia et al. 2006, Wang et al. 2014, Khoury et al. 2022). In individual of these studies, age >65 years, female gender, and hemoglobin level <10 g/dL were also prognostically unfavorable. In addition, a SETBP1 mutation was shown to have a negative impact (Piazza et al. 2013, Khoury et al. 2022, Patnaik & Tefferi 2023). 30-40% of patients show transformation to AML (Wang et al. 2014).
MDS/MPN-N: Recommendation
It should be noted that according to WHO 2022, when a CSF3R mutation is detected, CNL should be excluded morphologically as part of the differential diagnoses. Similarly, if a JAK2, CALR or MPL mutation is detected, an accelerated phase of MPN should be excluded based on history.
In contrast, according to WHO 2022, the presence of a SETBP1 or ETNK1 mutation supports the diagnosis of MDS/MPN-N (Khoury et al. 2022).
Status: June 2023